
How to market your Law firm to get more Personal injury clients
Unlock the full potential of your personal injury practice with the right clients – here’s how to attract and retain calls and cases.
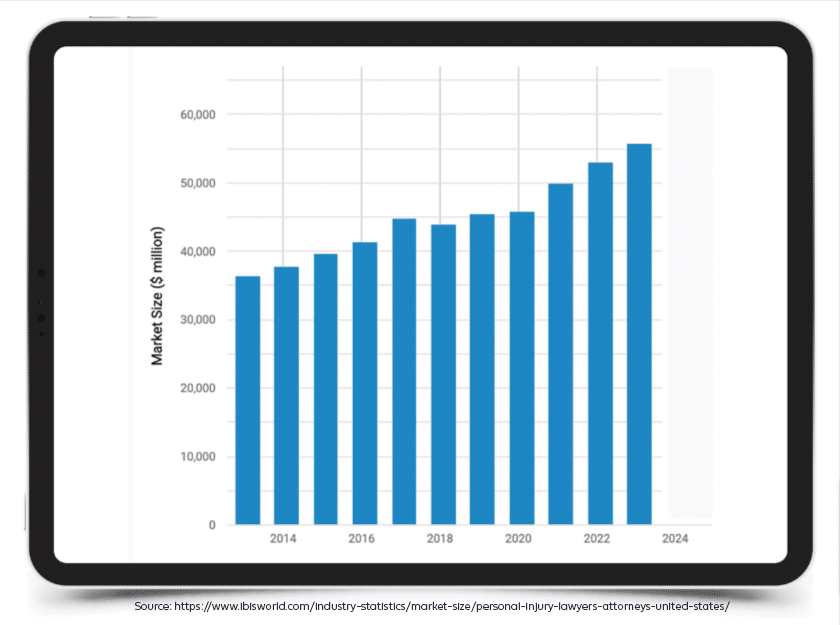
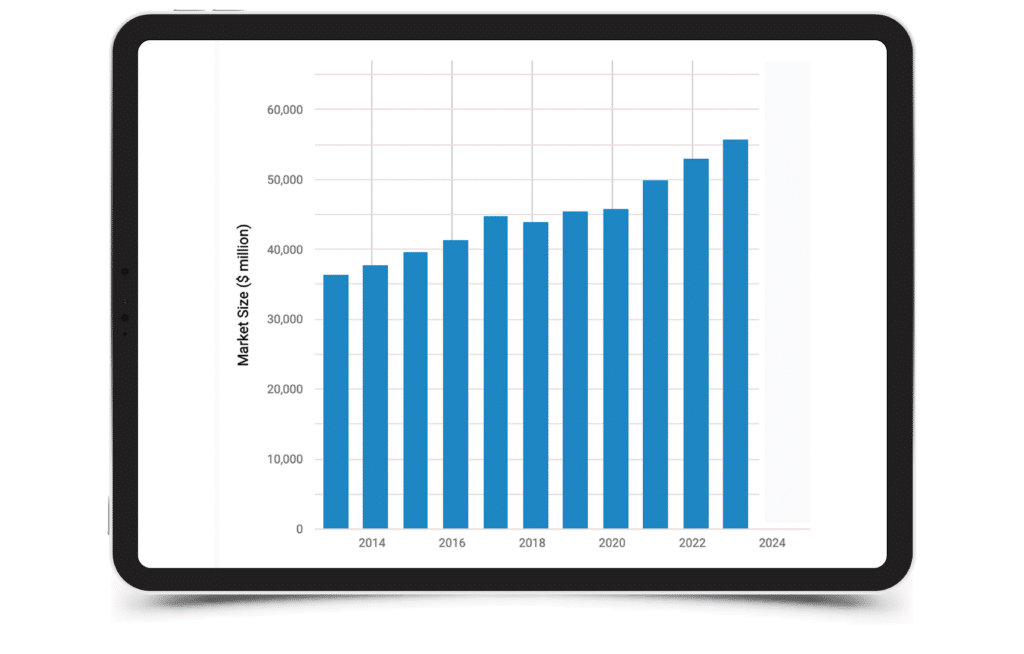
Did you know that studies found the market size of the personal injury industry in the US has grown an average of 4.8% per year between 2018-2023? Specifically, in 2023, the market size is expected to increase by 5%.
As a personal injury law firm, acquiring new clients and signing valuable cases is crucial for the growth and success of your business. However, the challenge lies not only in acquiring new PI clients but also in attracting the best and most valuable cases.
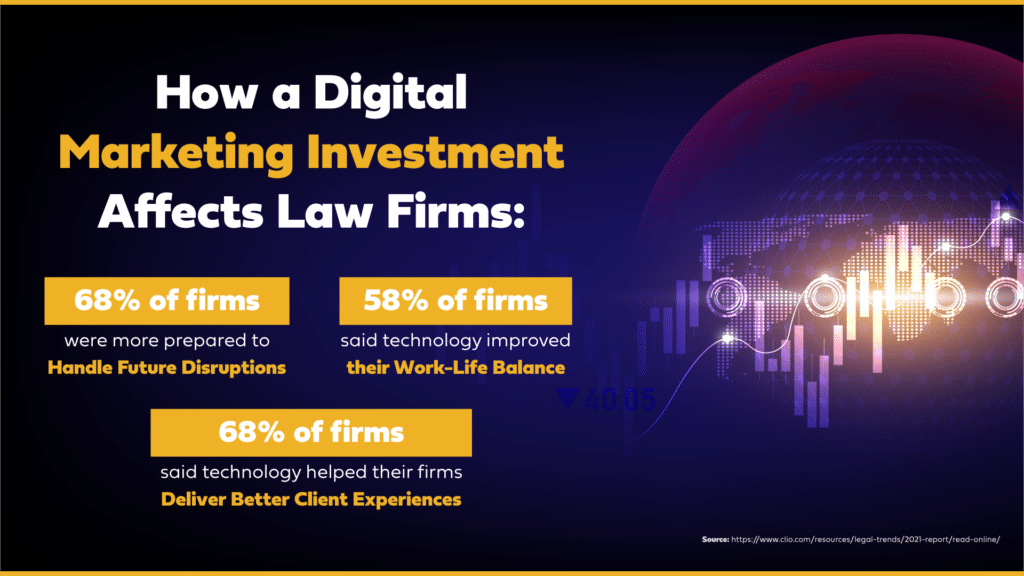
To boost bottom-line results and the overall image of an injury firm, many are investing more in digital ads in their personal injury marketing.
The task of acquiring new personal injury clients can be challenging, but you don’t have to figure it all out by yourself. If you are in search of a new marketing vendor, we can also help you out with our decision-making handbook, to guide you through this tough process:
Stay with us as we uncover a few clever strategies you can implement to attract and retain clients despite high-level competition.
Clever Ways to Get More Personal Injury Clients
-
Recognize Why Personal Injury Firms Fail to Scale
Do you know why your law firm practice isn’t growing? Despite rising costs, many firms fail to scale not because of monetary issues but because money isn’t managed in the smartest way possible. Here are 3 red flags you should be on the lookout for:
 Today, the smartest (and most profitable) Injury law firms are:
Today, the smartest (and most profitable) Injury law firms are:- Setting measurable goals that are aligned with the firm’s direction, purpose, and vision.
- Leveraging digital investments like PPC or Digital Advertising to activate both short and long-term sales.
- Driving their marketing, sales, and overall business strategy with data-driven decisions.
-
Secure Your Foundation
Niche down to scale up. But first things first: you’ll need to secure the foundation with a website. Think of your law firm’s website as your home. It not only houses everything your clients and prospects need, but it also houses all your creative assets such as videos, blogs, guides, ebooks, and pretty much anything you can think of!
We have pro-tips to get you started here:
- Think of factors that differentiate you from the rest of the competition. This is somewhat related to your business’s unique value proposition, the statement where you let prospects know:
- How clients benefit from your legal service(s)
- How your services address and solve their legal urgency. Niche down to scale up What makes your firm’s offer different than the rest
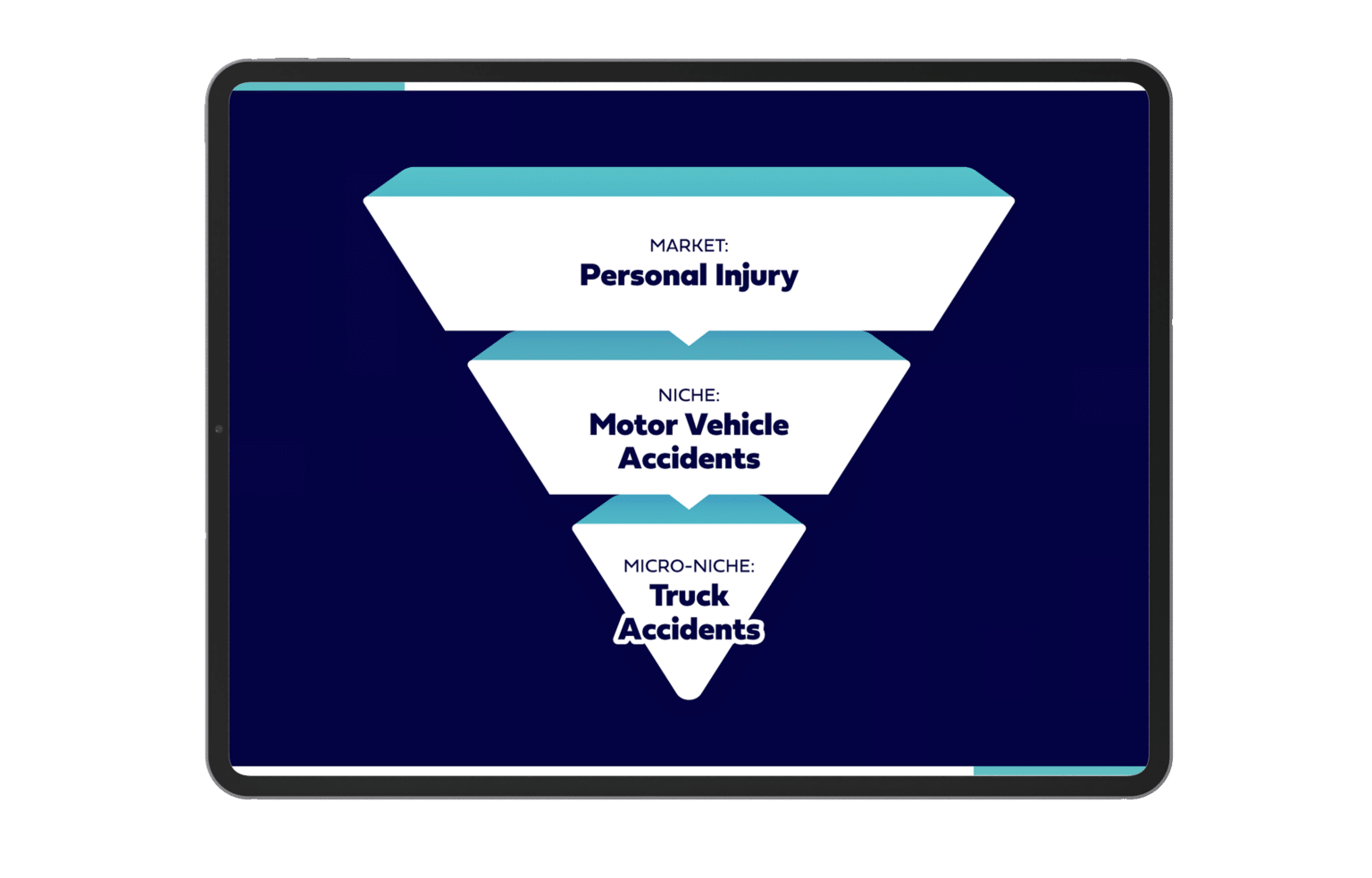
- Legal niche marketing works for many firms because it allows them to laser-focus on pre-defined, specific, and targeted audiences. To help you get started, think back to this question: What problems do you want to solve? Here’s an example of a personal injury micro-niche:

-
Fortify the Lead Intake Process
The legal intake process is considered a vital aspect of a law firm. Receiving a lead is a huge business opportunity that shouldn’t go to waste!
To help you secure more business, feel free to check out our guide with the 9 proven lead intake tactics.
We’ll give you two tips now:
- Make sure you discuss your payment process and accepted methods of payment.
- Ask the right questions. For example, you’ll want to ask questions related to the likelihood of the lead converting to a case.
-
Need to Boost Your Lead Pipeline? Protect the Intake Process
Besides securing the lead intake, you’ll want to consistently nurture your lead pipeline. For starters, you’ll want to optimize your website to convert the most leads. Here are some best practices for that:
- Use simple language, avoid legalese, and legal jargon
- Keep the copy visually appealing by adding bullets….like this!
- Add a mix of images and videos
- Add calls-to-action
- Above all, provide value

Personal Injury Law Marketing Insights
When looking for a lawyer, potential clients not only want quick answers but also want to be confident they’ll be in the hands of the very best. This is why they’ll deep dive, researching each firm before making that crucial decision. This is where a standout website and an engaging online presence come into play.
Your website and digital assets should catch prospects’ attention to ultimately convert them into calls and cases.
Every personal injury case is unique, which means the plan of action will depend on many moving variables, including but not limited to:
- What’s the type of injury?
- How did it happen?
- Where did it happen?
While personal injury is one of the most competitive fields in law, you can truly rise above the competition by:
- Highlighting your expertise in areas specific to your practice.
- Engaging clients right from their first search.
Remember, effective personal injury marketing companies are about:
- Connecting
- Showcasing
- Reassuring
If you’re interested in knowing how to get personal injury clients and understand how potential clients choose the best personal injury lawyers, check this out!👇
Personal Injury Marketing Customer Experience
After a car accident, victims often feel shocked, lost, and in need of help. During these times, there’s a predictable pattern victims do— they search for trusted legal representation online.
Car accidents remain a dominant practice within personal injury law, and this makes the competition among law firms more intense. As a matter of fact, the personal injury market is set to grow by 5% in 2023 compared to 2014. Take a look at these findings:
While other victims might call their families and friends for attorney recommendations, many will still instinctively turn to online searches to look for attorneys with the best reviews and strong credentials.
This is where having a great personal injury law firm marketing is mostly needed.
In this digital age, word of mouth won’t suffice anymore. Firms must stay ahead of the game by having clever online marketing strategies. Let’s delve into how marketing your personal injury law firm truly influences a victim’s journey from the crash scene all the way to your office.
So, to start, let’s dive into the client’s behavior…
How Clients Select Their Personal Injury Attorney After a Car Accident
All clients have a standard that they want to meet when choosing the best personal injury lawyer that will represent them. They want to be in the hands of the very best.
What are the common denominators?
Here are some of the basic things they look for.
- Experience in representing a car accident victim.
- Proof of relevant experience, such as case studies or testimonials showcasing their successful work.
- An approachable personality that makes them feel you’re someone they can talk to.
Uncover the full details by watching this LAWsome episode with Ken Hardison, founder & president of PILMMA, The Personal Injury Lawyer Marketing & Management Association:
Now that you have a better understanding of what clients look for when searching for a personal injury lawyer, let’s dive into how you can place your firm in front of your competitors.
Top Personal injury Digital marketing Strategies
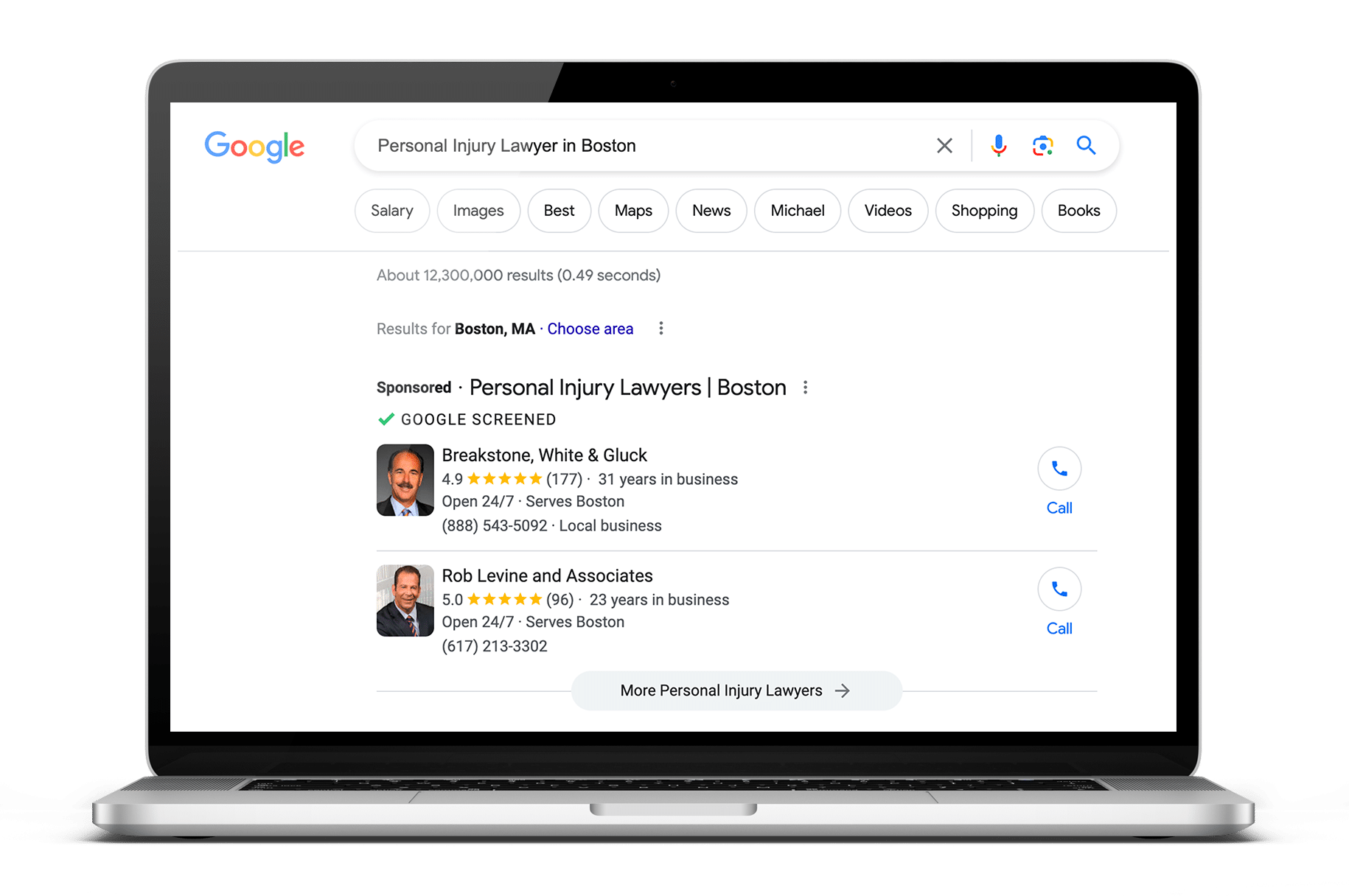
Google Local Services Ads
LSAs, local services ads, help firms generate personal injury leads that can turn into clients.
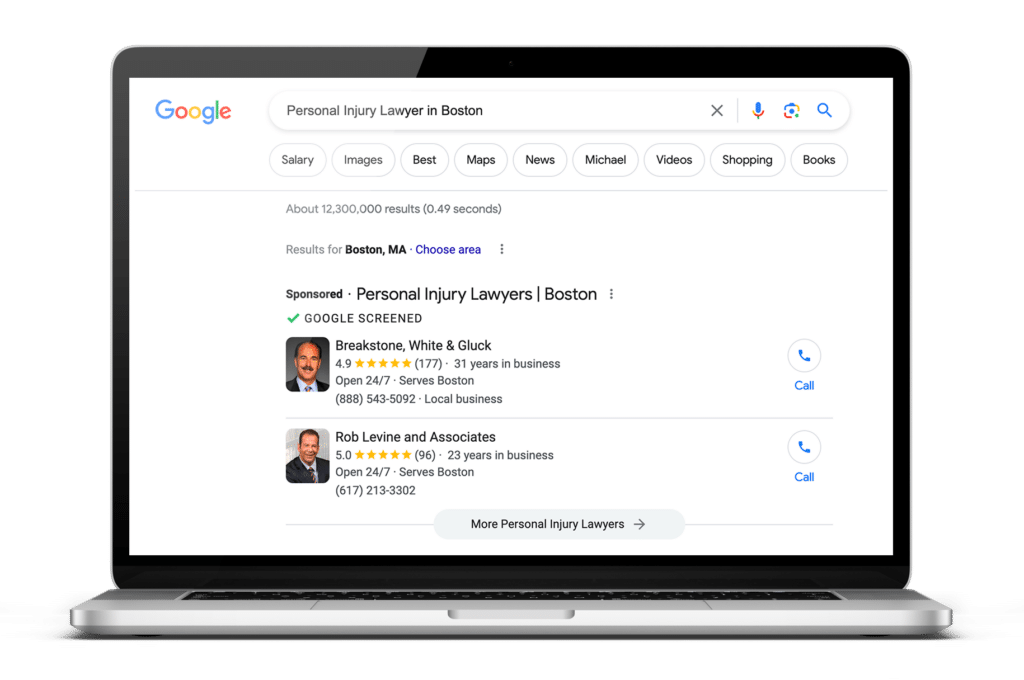
The main goal of LSAs is to make your law firm appear to prospective clients searching online in your area for the services that you offer. It will help your firm’s profile or the lawyer representing your firm to show at the top of Google’s search results.
The local ads are Google screened, providing the searchers with valuable information, such as your reviews and years in business. Here’s an example:
What LSAs Can and Cannot Do
- LSA is pay-per-lead, unlike PPC, which is Pay-Per-Click.
- You only pay once someone calls your firm by clicking on the phone number listed on the LSA post.
- It has a “click-to-call” feature.
Now, let’s find out why PPC is also one of your firm’s best options in successful personal injury law firm marketing.
Personal injury Law firm PPC
With PPC for law firms, firms can bid on specific keywords relating to their services.
In search engine results, the law firm might appear at the top or in a visible area if the user searches for those keywords. By clicking on the ad, the law firm pays a fee to the search engine (Google, Bing, YouTube, etc.). As a result, law firms can target potential clients actively searching for their services. When it comes to car accident cases, usually the urgency is immediate, so it is vital your firm is ready to offer a helping hand.
Other personal injury law firms working with Consultwebs have seen results from this.
Just look at how Consultwebs helps a law firm reduce its cost-per-lead by more than half using a PPC campaign in this case study:

In addition to keyword research, the Consultwebs team created new ad groups and wrote new copy for the advertisements. Despite spending less, the cost per lead dropped from $301 to $129, and the firm saved $7000 over 3 months.
You can also master Pay-Per-Click advertising for law firms – start by diving into this video:
https://www.youtube.com/watch?v=GjIXww7JyEg&t=319s
Personal injury SEO
Car accidents are unpredictable, but they happen. Fortunately, you can be there to help 24/7.
If your law firm is looking for wider visibility, long-term online growth, more calls, clients, and cases, then Personal injury lawyer SEO should be your go-to strategy.
Search engine optimization will provide your firm with long-term benefits such as:
- Enhancing your website by optimizing it to appear in Google’s SERPs
- Concentrating on Local SEO
- Merging Off-page SEO and On-page SEO
- Boosting your local traffic
- Boosting your online reviews
- Improving social media management
- Performing continuous keyword optimization
- And so much more.
Be There When Car Accident Victims Need Your Firm the Most
No one should go through car wrecks alone. As an experienced law firm, you can take steps to be there at the right place at the right time.
This is why many personal injury law firms are diversifying their strategy by investing in different digital assets.
Car accident victims shouldn’t settle for less, and neither should your firm’s business. This is why personal injury law firms are partnering with Consultwebs.
Take a look at another client case study:
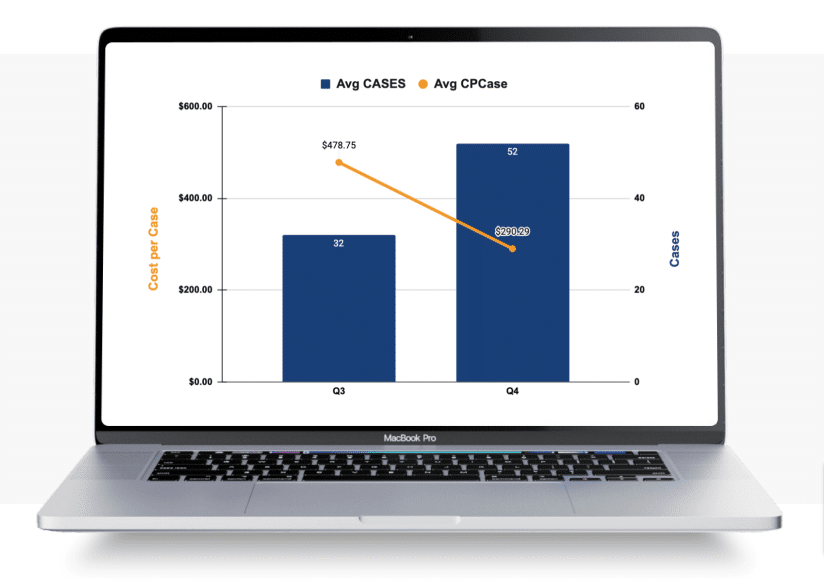
The data is between Q3 and Q4, the firm has managed to:
📈Increase the number of cases by 62.5%
📈Decrease cost per case by 39.7%
Marketing personal injury shouldn’t be complicated; let us guide you to success.
Read the Rest of the Case Here.
Building Trust with Clients
The personal injury market is growing. Learn why law firms should explore new strategies to grow their business.
When it comes to building a successful law firm, trust is everything. Imagine walking into a store and not trusting the salesperson to give you accurate information, or a doctor not earning your trust before performing a procedure. The same applies to the legal industry; clients will look for representation elsewhere without trust. But how do you establish trust with potential clients in a competitive market? How can you identify the gaps within your business?
To answer this question, we need to take a step back and analyze where clients find, compare, and ultimately choose a law firm nowadays?
Let’s take a look:

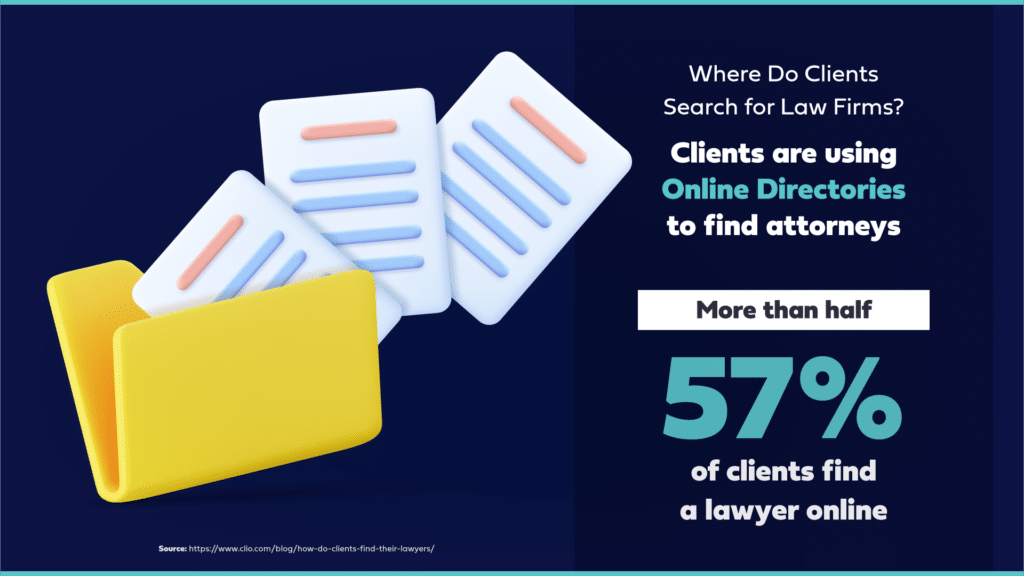
Where would you search for a lawyer? Put yourself in the client’s shoes. Legal services are a high-ticket purchase, and you would want to be in the hands of the best. So while you may start by asking your circle of friends and family for possible legal referrals, there’s also a high chance you’d go online and check Google reviews, testimonials, etc.
What does this all mean? Personal recommendations are influential, but online research is equally (if not more) important.
Personal Injury Marketing is Growing. Is There Untapped Potential?
The personal injury market is set to grow by 5% in 2023. Take a look at the findings:
This market growth is an excellent thing for both clients and firms. It is also driving more firms to secure increased business through a mix of digital marketing strategies. Want more information about our thoughts on 2023 trends and predictions?
But why should your firm keep up?
- Reach a wider audience: If you’re not boosting your online presence, but your competitors are, there’s a chance clients will keep your competitors top of mind instead of you.
- Establish expertise: Know of any updates in law? Building on high-quality content helps establish your firm as the expert.
- Personalization: Want to be memorable? Create a unique customer experience. Clients today want to be something other than a number in your books; they want to feel special and seen.
- Enhance your reputation: By providing valuable content, maintaining a social media presence, and investing in a high-quality website etc., you will truly build a positive (and sustainable) reputation.
- Stay competitive: As the personal injury market grows, you can set yourself apart from the rest and target the people who need you through consistent marketing.
- Build relationships: In business, relationships are everything. With the help of social and email marketing, you can nurture relationships with prospects and clients.
- Improve your client retention: Did you know that acquiring a new customer costs 5X more than retaining one? Retention is key.
The most critical reason for firms to keep up is to build trust.
Find Out Why Trust Is The Key For Profitable Firms
Digital Marketing Strategies Proven to Boost Profitability
Firms can establish their expertise, reliability, and credibility with a mix of the following assets:
- High-quality website: A professional and well-designed law firm website can establish a firm’s credibility and expertise. It can also provide potential clients with information about your firm’s services and attorneys, building trust and confidence in its abilities.
- Valuable content: Creating helpful and informative content such as blog posts, infographics, and white papers can establish a firm as a thought leader.
- Testimonials and reviews: Positive testimonials and reviews from previous clients can be a powerful way to build trust as they showcase your track record of success and client satisfaction.
- Social media presence: An active presence can help law firms build trust with potential clients by showcasing the firm’s personality and humanizing the attorneys.
- Email marketing: Email marketing can reach clients directly in their inboxes and provide them with valuable information.
- Digital advertising: Digital advertising methods such as Google Ads, Facebook Ads, and LinkedIn Ads can help you target specific audiences in your legal jurisdiction.
- SEO: Search Engine Optimization uses various optimization strategies, e.g., adding links, keywords, and publishing quality content. All of this signals search engines and prospects that your website is valuable.
Examples of Personal Injury Claims
There are different injury claims that fall under personal injury law, and the ideal marketing approach is different for each type of personal injury case your firm wants to target.
Here are a few of the primary practice areas that fall under personal injury:
Motor Vehicle Accident Injuries
Marketing Motor Vehicle Accident Injuries in law firms is distinct due to the targeted outreach to victims seeking timely legal recourse for complex, often traumatic incidents. If you want to get some ideas on how to reach motor vehicle accident clients, follow the link.
Workplace Injuries
Marketing Workplace Injuries in law firms is unique because it addresses the nuanced intersection of employee rights, employer responsibilities, and intricate workers’ compensation laws.
Although Workplace Injuries Marketing has to consider many factors, law firms still need to prioritize the importance of focusing on a legal niche when marketing a law firm. Learn how niche targeting can make a difference and how to choose the right niche by watching this Podcast!👇

Assault, Battery & Willful Violence
In law, assault typically refers to the threat or attempt to inflict physical harm, battery is the actual physical harm inflicted on another person without their consent, and willful violence denotes intentional, aggressive behavior that causes or aims to cause harm.
The deeply personal nature of such cases necessitates a marketing approach centered on trust, sensitivity, and swift justice.
Defamation: Libel And Slander Defamation
These practices involve damaging one’s reputation through false statements, whether written (libel) or spoken (slander). Marketing here hinges on the value of reputation and the ability to defend one’s name assertively.
Premises Liability
This area covers injuries occurring on someone else’s property due to negligence. Distinctive marketing emphasizes the responsibility of property owners and the right to safety for all visitors.
Wrongful Death
Marketing for Wrongful Death cases requires addressing the profound grief of families while emphasizing the pursuit of justice for lost loved ones.
Product Liability
Law firms marketing product liability services should position themselves as expert defenders of consumer rights and advocates for those harmed by defective or dangerous products.
Medical Malpractice
Medical malpractice occurs when a patient is injured because of negligent medical care. A case can be made when mistakes are made during diagnosis, the application of anesthesia, surgery, and/or faulty drug prescriptions, and more.
- Examples: dental medical malpractice, birth injury medical malpractice.
Personalized Personal injury Marketing strategy for your Law firm
At Consultwebs, we recognize the effects one factor has on another. We take a comprehensive marketing approach and tailor it to your firm’s wants and needs, and we deliver results. We are not your average digital marketing team. Our experts focus entirely on the legal industry, so you can expect to stand out amongst your competitors through our specialized marketing approach that caters to Personal Injury law firms:
Search Engine Optimization
(SEO) can give you plenty of local and regional opportunities, as well as a competitive edge. A sturdy SEO campaign can boost your rankings and placement on the Google SERP, which will increase your chances of being found by the right prospects at the right time. The main advantage of SEO is being found without having to pay for clicks. It is free, organic marketing.
SEO for personal injury lawyers is most efficient when implementing a Local SEO Strategy.
Pay-Per-Click Advertising
In today’s digital era, visibility on online platforms is crucial for any profession, and personal injury lawyers are no exception. Digital ads tailored for personal injury lawyers are designed to target potential clients who might be searching for legal assistance online after experiencing an injury or accident.
Using advanced targeting techniques, these ads can appear on search engines, social media platforms, and other digital spaces where potential clients might be. The key benefit is immediate visibility; as soon as someone looks for relevant help, the lawyer’s ad promptly appears, presenting a solution.
Social Media
Social media can help you reach out to potential clients and engage with your current ones. By creating a strong social media presence, you can increase your brand awareness, promote your services, and showcase your expertise in personal injury law.
Video Marketing
Video marketing is an effective way to communicate with potential clients and build trust. You can use videos to explain complex legal concepts, share client testimonials, or showcase your firm’s culture and values.
Podcasting
Podcasting allows you to reach out to a wider audience and establish yourself as an industry thought leader. By sharing your insights and experiences, you can build a loyal following and attract more potential clients to your firm.
Web Design
Your website is the face of your personal injury law firm online. It’s where potential clients will go to learn more about your services and decide whether to contact you. That’s why it’s important to have a website that’s not only visually appealing but also user-friendly and informative. A well-designed website can help your firm stand out from the competition and ultimately generate more leads.
Content Marketing
Content marketing is the practice of creating and sharing informative and valuable content to attract and engage a targeted audience. By creating high-quality blog posts, articles, and other types of content, you can position your personal injury law firm as an industry leader and build trust with potential clients. Content marketing can also help your firm rank higher in search engine results pages (SERPs) and ultimately generate more leads.
Email Marketing
Email marketing remains one of the most effective ways for personal injury lawyers to stay connected with potential and former clients. This service offers lawyers the ability to send targeted emails to individuals who might be in need of their legal expertise following an injury.
Well-crafted email campaigns can provide valuable information on what to do after an accident, share client testimonials, or update recipients on recent case victories. Besides nurturing leads, email marketing also helps establish a strong professional rapport and ensures the lawyer stays top-of-mind when legal services are needed.
Accident Data Center
The Accident Data Center serves as an invaluable repository of data and information related to various accidents and injuries. Personal injury lawyers can leverage this center to access detailed accident reports, witness statements, and other vital pieces of evidence that can strengthen their client’s case.
By having a centralized platform with such a wealth of information, lawyers can save time on research, build compelling cases with concrete data, and better understand accident trends, which can inform their future legal strategies.
Over-the-Top Marketing
Over the Top (OTT) Marketing, also known as Stream advertising, refers to marketing strategies that go beyond traditional methods, often utilizing modern digital platforms and unconventional tactics to create maximum impact in popular streaming platforms like:
- Hulu
- Roku
- Amazon Fire
- Apple TV
For personal injury lawyers, OTT marketing includes high-quality video content, interactive web platforms, or aggressive social media campaigns. The idea is to create a memorable brand presence that stands out in the crowded legal marketplace.
And there you have it! You surely have a better understanding now of personal injury lawyer marketing strategies.
Choosing the Right Marketing Agency for Your Personal Injury Law Firm
At Consultwebs, we deeply understand the distinct hurdles that personal injury law firms encounter in the digital marketing realm. Our specialized team, skilled in the legal sector, is poised to craft a custom marketing strategy tailored to your firm’s unique requirements.
Your success is our metric. We focus on the most important metric of them all: Return On Investment (ROI).
Our mission?
Help your personal injury law firm harvest more leads and expand your horizons.
Ultimately, we understand words aren’t enough – results should speak more than anything, which is why we believe in showcasing tangible results.





{kind=link}